

By Dhanvi Mathur/MAY 29, 2026
Few techniques in laboratory medicine are as durable, adaptable, and clinically valuable as the enzyme-linked immunosorbent assay. Since its development in the early 1970s, ELISA has become one of the most widely performed immunological assays in clinical laboratories worldwide, used to detect hormones, infectious agents, cancer biomarkers, and, critically for autoimmune diagnostics, specific autoantibodies in patient serum.
The global enzyme immunoassay market reflects the depth of that reliance. Valued at over $18.51 billion in 2025 and predicted to reach approximately $27.34 billion by 2035, the demand for reliable, high-throughput enzyme immunoassay solutions continues to expand alongside the growing prevalence of autoimmune disease and the increasing need for specific, quantifiable autoantibody data to guide clinical decisions.
Yet, not all ELISA test kits are the same. ELISA performance depends on far more than a reactive result; it demands consistency across lots, validated antigen substrates, calibrated controls, and matched reagent systems that function as a single integrated system.
For clinical laboratories managing high volumes of autoantibody testing, the difference between a well-designed ELISA immunoassay and a generic kit is the difference between diagnostic confidence and uncertainty.
This guide walks through how the enzyme-linked immunosorbent assay works, the four main types of ELISA, and where Immuno Concepts' RELISA® test systems fit into clinical autoantibody testing.
What Is an Enzyme-Linked Immunosorbent Assay?
An enzyme-linked immunosorbent assay is a plate-based immunological assay technique used to detect and quantify a specific substance, most commonly a protein, antibody, or antigen, in a biological sample. The core principle of ELISA relies on the specificity of antibody-antigen binding and on the measurable signal produced when an enzyme-labeled component reacts with a substrate, resulting in a color change.
In autoimmune diagnostics, the enzyme immunoassay format is used to detect autoantibodies: antibodies produced when the immune system mistakenly targets the body's own proteins. Because autoantibodies are directly associated with specific autoimmune conditions, detecting and quantifying them provides critical information for diagnosis, disease monitoring, and treatment assessment.
The result of a well-executed ELISA immunoassay is not merely a positive or negative signal. In quantitative and semi-quantitative formats, it is a calibrated value. This antibody unit tells the laboratory not just whether an autoantibody is present, but how much is present and how that level compares to established clinical thresholds.
The Four Main Types of ELISA
The enzyme-linked immunosorbent assay is not a single technique but a family of formats, each designed for different detection goals and sample types.
Understanding the distinctions between them helps laboratories select the right ELISA test kit for each application.
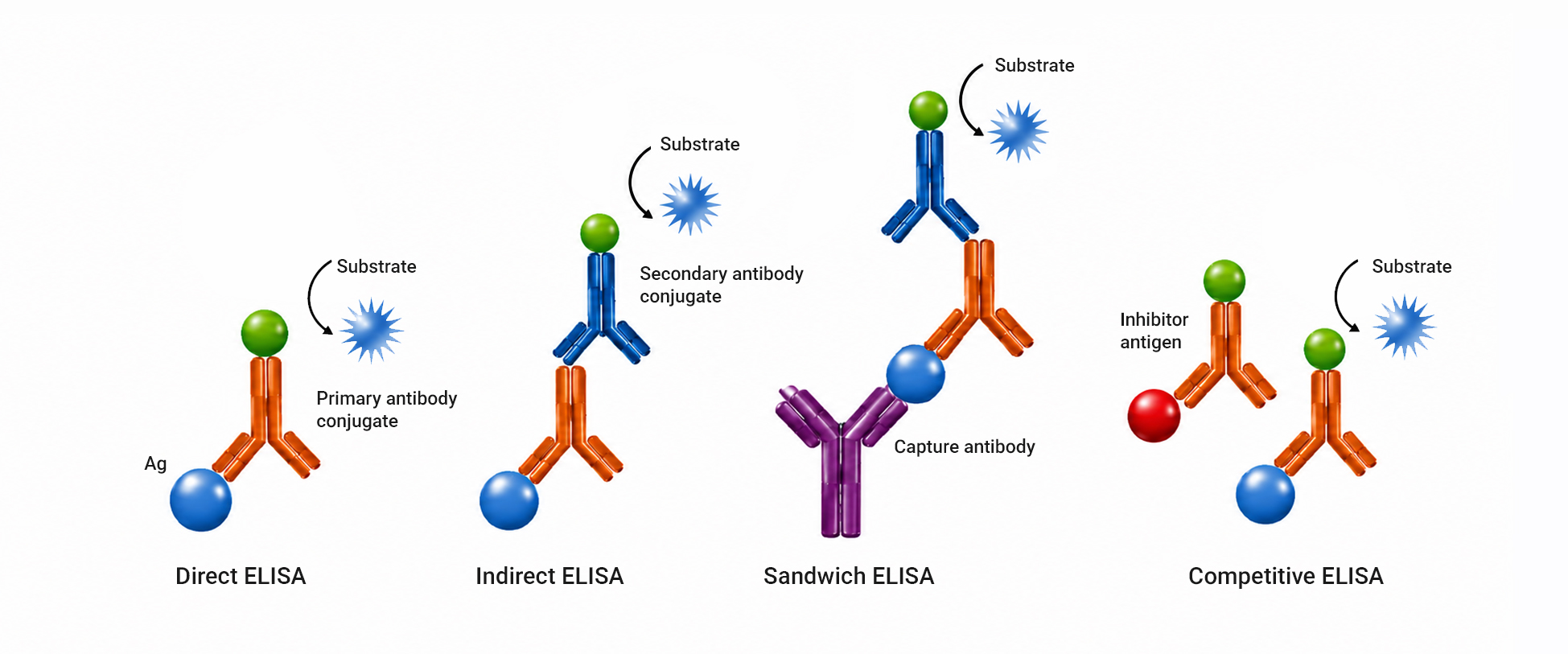
1. Direct ELISA
In direct ELISA, a potential antigen is immobilized directly onto the microplate surface. A primary antibody conjugated directly to an enzyme is then added, binding to the antigen and producing a measurable signal upon addition of the substrate. Direct ELISA is the simplest format and offers a fast workflow with fewer steps and less risk of cross-reactivity from a secondary antibody.
However, it is less commonly used in autoimmune clinical diagnostics because signal amplification is limited, conjugating every primary antibody to an enzyme is technically demanding, and it reduces assay sensitivity compared to indirect formats. Most importantly, the fundamental design is for detecting antigens, whereas clinical testing is more concerned with detecting disease-associated antibodies. Therefore, direct ELISA is more frequently used in research and antigen detection applications.
2. Indirect ELISA
Indirect ELISA is the most widely used format in autoantibody testing and ANA screening. The antigen is immobilized on the microplate, patient serum is added, and if the target autoantibody is present, it binds to the antigen during incubation.
A secondary antibody, conjugated to an enzyme and specific to human immunoglobulins, is then added, binding to the captured autoantibody and generating a signal upon substrate addition.
The key advantage of indirect ELISA is signal amplification. Because multiple secondary antibodies can bind to each primary antibody, the optical signal is significantly stronger than direct formats, improving sensitivity. This makes indirect enzyme immunoassay particularly well-suited to detecting low-concentration autoantibodies, a common requirement in early autoimmune disease, where autoantibody levels may not yet be markedly elevated.
Indirect ELISA is also highly adaptable. By changing the antigen substrate coating, the same assay format can be directed at any number of autoantibody targets.
Immuno Concepts leverages this format across the RELISA® test system portfolio because indirect enzyme immunoassay combines the sensitivity needed for reliable ANA screening with the flexibility to target a broad range of specific autoantibody applications. By using validated, in-house-produced antigen substrates in each microwell, Immuno Concepts ensures that the antibody capture step, the most variability-prone element of the indirect ELISA format, is controlled at the source, before the kit ever reaches the laboratory.
3. Sandwich ELISA
Sandwich ELISA uses two antibodies, a capture antibody and a detection antibody, to bind the target antigen from both sides, literally sandwiching it. The capture antibody is immobilized on the microplate surface. When the sample is added, the target molecule binds to the capture antibody. The detection antibody, which is enzyme-labeled or detected by a secondary enzyme-labeled antibody, then binds to a different epitope on the same target.
Sandwich ELISA offers extremely high specificity because the target must bind simultaneously to two antibodies. It is the preferred format for antigen detection, measuring cytokines, growth factors, hormones, and pathogen antigens, whereas for autoantibody detection, the patient's own antibody is the target rather than a foreign antigen.
In clinical laboratories performing autoimmune diagnostics, sandwich ELISA is more commonly encountered in research applications or in assays designed to quantify specific proteins associated with inflammatory activity.
4. Competitive ELISA
Competitive ELISA, also known as inhibition ELISA, operates on a different principle from the three formats above. A known quantity of labeled antigen competes with the unlabeled antigen in the patient sample for binding to a fixed number of antibody sites. The more antigen present in the patient sample, the less labeled antigen binds, meaning the signal produced is inversely proportional to the concentration of the target in the sample.
Competitive ELISA is particularly useful for detecting small molecules and haptens that cannot be bound simultaneously by two antibodies, as required in sandwich formats. It is also used in certain autoantibody detection contexts where high-affinity binding is required. The format offers robustness in complex samples where matrix interference could otherwise affect results, though its inverse signal relationship requires careful calibration and interpretation.
With the four ELISA formats in view, it becomes clear why indirect enzyme immunoassay is the clinical standard for autoantibody testing, but how that format is executed matters just as much as which format is chosen. Here is how Immuno Concepts' RELISA® test systems put that into practice.
Why ELISA Is Central to Autoimmune Diagnostics
The enzyme immunoassay format has become indispensable in autoimmune diagnostics for reasons that go directly to the clinical needs of laboratories managing systemic rheumatic disease testing.
ELISA is quantitative. Unlike binary immunological assays, a well-designed ELISA test kit provides a calibrated antibody unit value that indicates the amount of autoantibody present, not just whether it is detectable. Rising anti-dsDNA levels can signal an impending lupus flare before clinical symptoms appear. Declining anticardiolipin titers can confirm treatment response in antiphospholipid syndrome. This longitudinal, quantitative dimension is what makes the enzyme immunoassay clinically valuable beyond initial diagnosis.
ELISA complements IFA. In standard autoimmune diagnostic practice, ANA screening by indirect immunofluorescence identifies whether antinuclear antibodies are present and reveals the ANA pattern, homogeneous, speckled, nucleolar, centromere, and others, that guides the next step. Positive ANA screen results are then reflexed to ELISA test kits for specific autoantibody identification and quantification.
ELISA scales. High-throughput microplate formats allow laboratories to process large volumes of patient samples in a single run, making enzyme immunoassay well-suited to both high-volume clinical screening and focused confirmatory testing without compromising turnaround time.
How RELISA® Fits Into the Autoimmune Testing Workflow
The RELISA® portfolio from Immuno Concepts is designed specifically to meet these three clinical requirements.
The quantitative output of RELISA® assays is supported by matched calibrators, validated lot-release thresholds, and in-house antigen production, which keep optical density performance consistent run after run, ensuring that the antibody unit values your laboratory reports are clinically meaningful and longitudinally comparable.
The RELISA® portfolio is designed specifically to function within the two-step IFA plus ELISA workflow. The RELISA® ANA Screen explicitly recommends reflex testing using Immuno Concepts' HEp-2 or HEp-2000® IFA slides for ANA pattern determination on positive results, creating a seamless, validated pathway from initial ANA screen to specific autoantibody confirmation within a single product ecosystem.
The RELISA® ENA Single-Well Screen directly addresses scalability demands, coating each microwell with six clinically significant antigens simultaneously, enabling high-volume laboratories to exclude ENA-negative samples cost-effectively before committing to specific confirmation testing.
Want a closer look at the RELISA® portfolio and its role in modern ANA and ENA testing workflows?
How the RELISA® Works in Practice: The Stepwise Process
Across all ELISA formats, the core workflow follows the same fundamental logic: bind, wash, detect, measure. Immuno Concepts has designed every step of the RELISA® test system process to minimize variability and maximize the clinical reliability of the result.
Step 1: Sample Incubation
Patient serum is diluted and added to antigen-coated microwells. In RELISA® assays, each microwell is coated with in-house, well-characterized antigens, ensuring consistent antibody capture and reproducible optical density across every lot. If the target autoantibody is present, it binds to the antigen on the well surface during incubation. Unbound antibodies are removed by washing.
Step 2: Detection
An enzyme-labeled secondary antibody is added, binding to any patient autoantibodies captured. In RELISA® assays requiring isotype-specific detection, such as the Cardiolipin IgG & IgM kit for evaluation of antiphospholipid syndrome, separate conjugates are provided for independent IgG and IgM determinations. A substrate solution then triggers a measurable color change, with intensity directly proportional to the concentration of autoantibody.
Step 3: Reading and Reporting
The reaction is stopped, and absorbance is measured on a standard microplate reader. RELISA® test kits report results as calibrated antibody unit values rather than raw optical density readings, providing the laboratory with a quantifiable, clinically interpretable result that supports differential diagnosis, disease monitoring, and longitudinal autoantibody tracking.
Simple in execution. Uncompromising in standards. That is every RELISA® ELISA test kit.
The Right ELISA Test Kit Makes Every Result Count
The enzyme-linked immunosorbent assay has earned its place in clinical diagnostics because it delivers what autoimmune testing demands: quantitative, specific, and reproducible results that laboratories can report and clinicians can act on. Choosing the right ELISA test kit means choosing consistency at every step, from the antigen substrate to the final calibrated output.
Immuno Concepts has built that consistency into every RELISA® assay for over four decades. Ready to see what RELISA® can do for your laboratory's autoantibody testing workflow?